The Australian has reported that largely routine or administrative consultations – such as sick certificates, repeat scripts, and unnecessary diagnostic imaging – have caused a big blow-out in Medicare spending:
When health professionals were asked to identify areas of “low-value patient care” that should be prioritised as part of the review, administrative GP consultations were mentioned the most…
The burden of administrative tasks and paperwork, which could be reduced or given to non-medical staff, included providing certificates for patients to take time off work, repeat scripts for those on medication, and extended referrals for those being treated by a specialist…
In 2013-14, for every 100 patient encounters, there were 49.1 pathology referrals (an increase from 36.7 in 2004-05) and 10.9 referrals for diagnostic imaging (an increase from 8.3 in 2004-05).
Inappropriate diagnostic imaging was the third most often cited area of low-value care by health professionals — four times the rate for pathology — and 24 per cent of consumers reported themselves, or their acquaintances, being referred for unnecessary care. One consumer reported having multiple blood tests ordered by different doctors due to a breakdown in communication between clinics and the laboratory, while a parent said “my son has had an X-ray for a chest infection four times (and) also had four hip X-rays — he is only 20 months old”…
I have personal experience with such matters.
My wife has undergone breast cancer treatment for the past three years. Under her treatment program, she must visit an oncologist and surgeon at regular intervals as well as take several medications for the next 10 years (to prevent re-occurrence).
I also have a son with autism who periodically needs to see a pediatrician.
Despite both having chronic conditions that will require long-term care, we are required to see a GP periodically to renew referrals to these specialists – a purely administrative task. It makes absolutely no sense, and ends up costing both us and the medical system.
There is undoubtedly a lot of duplication and waste in the system that should be eliminated – either via reducing the need for repeat referrals, outsourcing low-level or administrative tasks to nurses, or other measures.
That said, the Government should also acknowledge that part of the reason for the blow-out in Medicare costs relates to the blow-out in the number of overseas-trained doctors (OTDs).
Recent research by Mike Moynihan and Bob Birrell from the Australian Population Research Institute showed that the number of doctors has easily out-paced growth in the population, driven largely by a conga-line of OTDs that enter Australia to work in a regional area only to then move to the already-oversupplied city once their mandatory term is up:
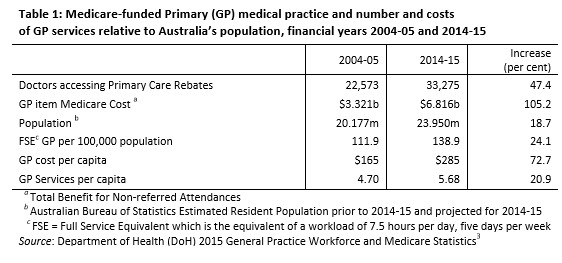
The number of GPs per 100,000 people in Australia far exceeds international benchmarks, especially in Anglophone countries. According to independent Australian assessments, by 2005 on this metric, there were already more GPs than was consistent with good medicine. Since then, as the following tables show, the number of GPs per 100,000 has increased sharply in metropolitan areas and even more so in some regional areas…
Given present policy settings, this oversupply will get much worse as many of the OTDs required to serve in undersupplied areas finish their service commitment and move into already oversupplied metropolitan or regional areas. Then to fill the gaps created by their departure, their employers recruit yet more OTDs to replace them…
As shown above, the number of doctors in Australia rose by 47% in the decade to 2014-15, around 2.5 times the 19% growth in the overall population.
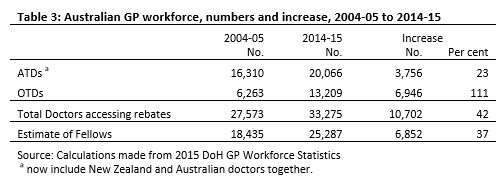
Moreover, much of this growth has come from OTDs, whose numbers have ballooned-out by a whopping 111% over this period. Most of these doctors are also practicing in over-supplied metropolitan areas, not areas of shortage:
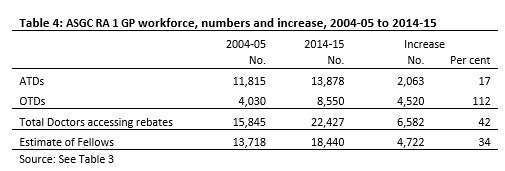
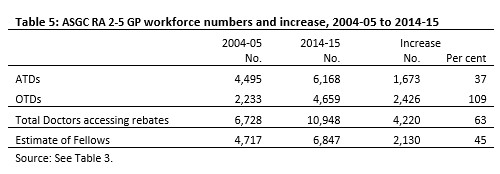
The purpose of the OTD promotion policy was to get more doctors into underserviced areas, particularly RA 2-5 areas. But Tables 4 and 5 show that most of the extra OTDs, by 2014-15, were practising in RA 1 areas.5 Of the total increase in OTDs (6,946) shown in Table 3, 4,520 were practising in RA 1 areas and 2,426 in RA 2-5 areas.
What has happened is that there has been a gradual leaching of OTDs into RA 1 areas where there is an ample supply of doctors, as well as into the more attractive provincial cities such as Ballarat, Bendigo and Shepparton in Victoria, where the situation is similar…
Alarmingly, the report notes that OTDs are not only responsible for much of the doctor oversupply, but also the blow-out in Medicare rebates:
The OTDs influx is therefore responsible for most of the growing oversupply of GPs in RA 1 locations. They are also responsible for most of the increase in Medicare service costs. By June 2015, for all of Australia, OTDs made up 39.7 per cent of the workforce but received 49.8 per cent of total rebates. In RA 1 areas they made up 38.1 per cent of the total workforce and received 47.6 per cent of services paid for by Medicare.
The consequences of which are a continued blow-out in bulk-billed GP visits and Medicare funding costs.
Controlling Medicare costs requires more than just the elimination of wasteful practices, but also reining in the 457 visa rort that has oversupplied our cities with GPs.
Leith van Onselen is Chief Economist at the MB Fund and MB Super. He is also a co-founder of MacroBusiness.
Leith has previously worked at the Australian Treasury, Victorian Treasury and Goldman Sachs.